This blog covers the presentation given as part of the ISPOR pre-conference plenary session on HEOR in the era of COVID-19 which was held on 14 May 2020. The video for the full session, including the panel of which this presentation was a part, can be found on the ISPOR website.
Thank you to the organizers for the invitation to talk today. It’s a pleasure to join this panel and tell you a little about the work we have been doing related to the health burden impact of COVID-19 fatalities.
One thing that I have learned as an HEOR modeler is that infectious disease modelling is a specialist activity that is best left to the experts. That’s not to say that we do not have those experts as part of our HEOR community – but simply an observation that the majority of HEOR and cost-effectiveness modelling are static models. Therefore, I would argue that for most of us, the focus should be on ‘layering’ by adding additional information to increase the richness of the epidemiological models and help turn them into full policy/economic models.
For instance, most epidemiological models stop at predicting lives saved from different mitigation strategies for handling the pandemic. While it is clear from the emerging evidence that victims of COVID-19 tend to be older and tend to have existing long term conditions, what is not clear is how to interpret this information. Unfortunately, this information has led some to suggest that these fatalities are occurring among those that ‘would have died anyway’.
To inform the debate, we have been working on a simple model to summarize the quality adjusted life years lost due to COVID-19 fatalities. Our starting point was a standard life table analysis which we adapted in three ways. First, we added a parameter for the standardized mortality ration (SMR) that allows for increased risk of death due to the existence of comorbidities. Second, we quality-adjusted the life-years by applying age-specific quality of life norms together with a further decrement for the existence of comorbidity. Finally, we discounted to give a net-present value of discounted QALYs lost.
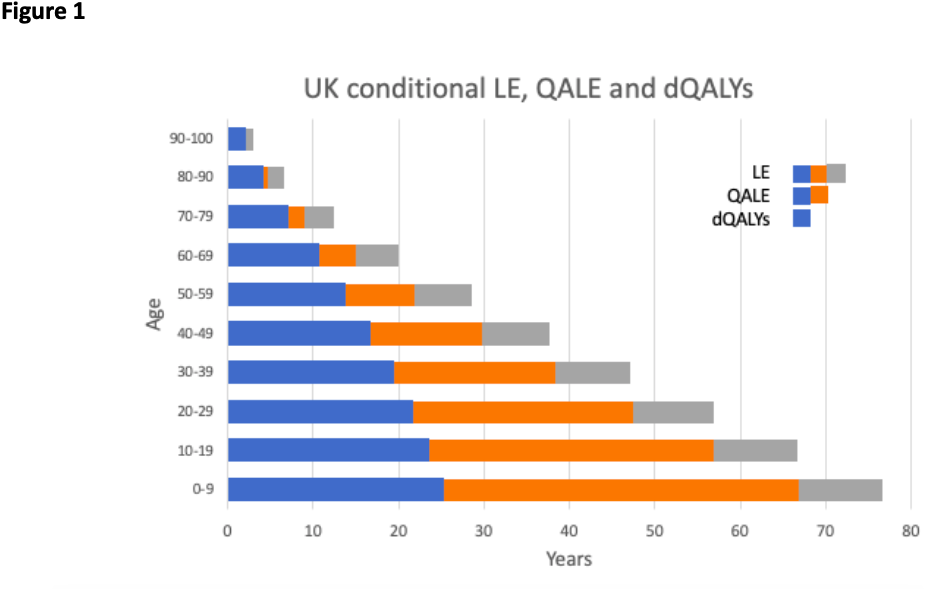
Figure 1 shows the results for the UK in terms of life-expectancy (LE), quality adjusted-life expectancy (QALE) and discounted QALYs (dQALYs) by age, assuming a SMR of 1, which is equivalent to no excess comorbidity (life tables already include the ‘average’ background levels of comorbidity in the population). The figure shows that age I highly predictive of reduce life expectancy and that discounting reflects a major adjustment for younger ages, but has very little impact on the estimates for older ages.
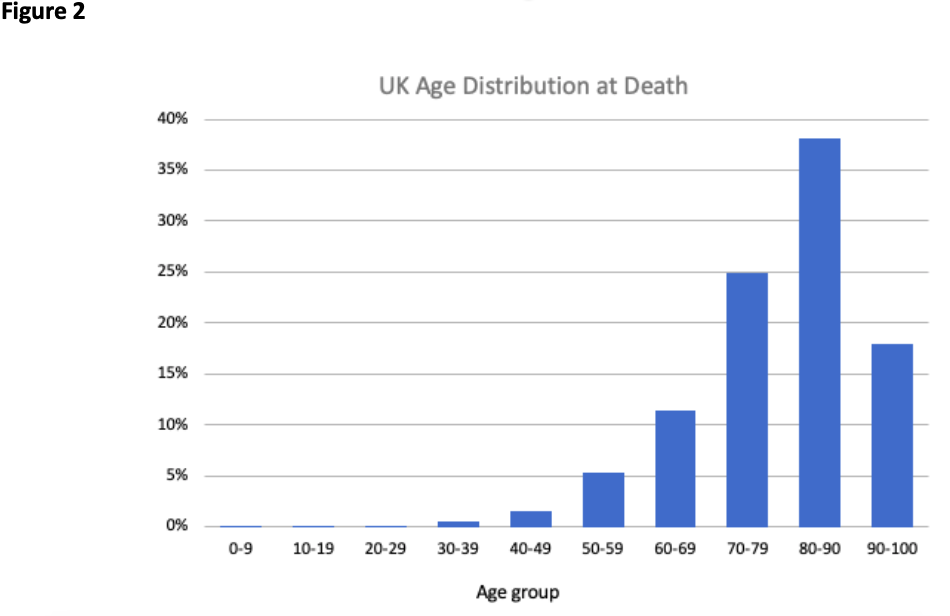
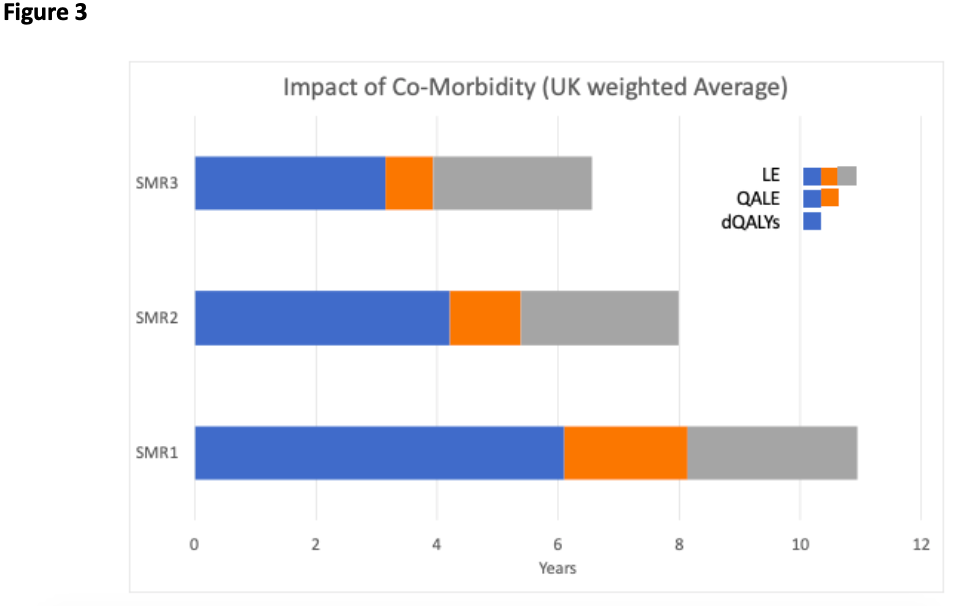
Once we have the conditional quantities, we can then generate a weighted average for a COVID-19 fatality by weighting according to the age distribution at death. The age distribution at death is shown in Figure 2 for the UK, based on data published by the UK Office of National Statistics. These data are regularly updated and are available on the ONS website. Using the weighted average quantities based on combining the information in Figures 1 and 2 we can look at the impact of comorbidities as presented in Figure 3. As the SMR increases the quantities reduce, as expected. Quality adjustment has the same net effect across different levels of SMR, while discounting is less important as SMR increases (as greater life expectancy is discounted more heavily).
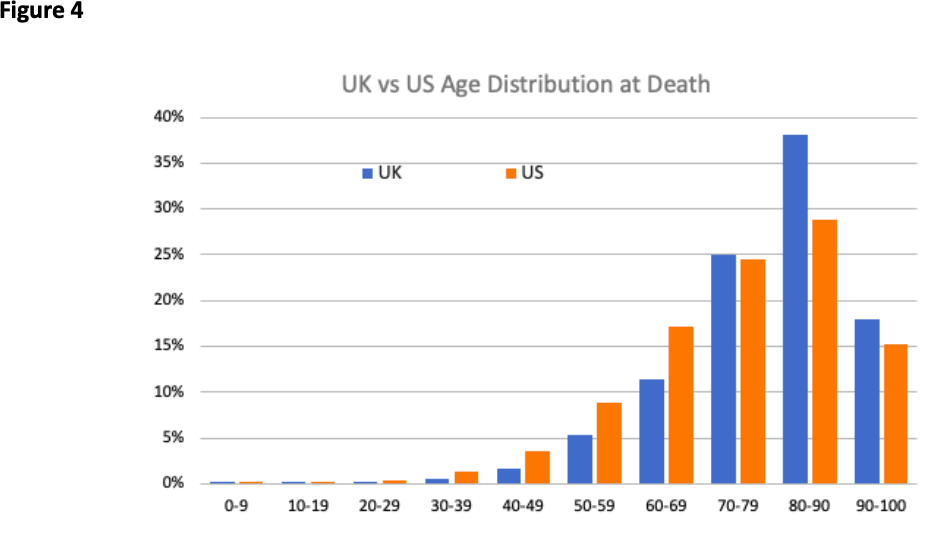
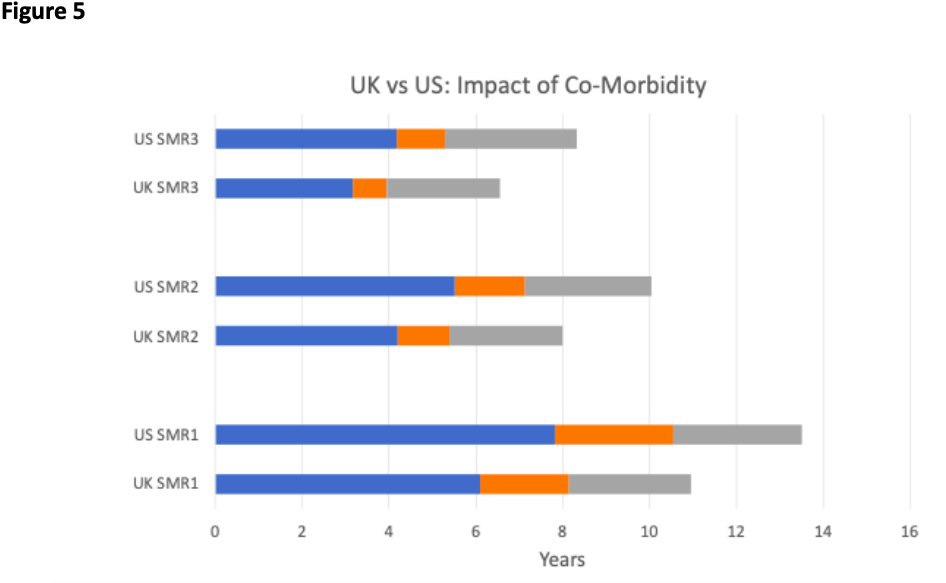
The relative simplicity of the tool facilitates international comparisons. In Figure 4, we show the age distribution of death in UK contrasted with the US. COVID-19 victims in US are relatively younger and this has the consequence that all estimated quantities are higher for the US than the UK as is shown in Figure 5.
Although in demonstrating the use of the tool we have concentrated on the direct impact of COVID-19 fatalities, it is important to note that the tool can also be used to examine the impact of indirect effects. For example, much interest has recently been focused on the potential health effects of delays to routine treatment as health care resources have become dedicated to addressing the pandemic. In particular, the health consequences of lockdown and other social distancing measure on immunization uptake could be dire. Furthermore, a number of commentators have speculated that the economic consequences of the pandemic could result in lives lost due to the relationship between wealth and health. Combined with the costs of alternative mitigation strategies, the tool presented here could help in moving towards a full economic evaluation of different policy choices.
Full details of the method can be found in this accompanying technical note and the method is implemented for (currently) five countries in this spreadsheet tool.
(By Andrew Briggs)