Some time has passed since we began writing in Issue Briefs about the distinction between charged amounts, or prices, and reasonable, fair market value. In the field of economics, these distinctions generally don’t pose a problem, because prices tend to gravitate to fair market value. In other words, if I own a coffee shop and I list a cup of coffee for $500, nobody will buy it at that price (that is, nobody would be “willing to pay” that amount), so I would begin to lower the price. We see this in housing markets, where sellers will begin lowering their asking price if no buyers are interested in buying at the list price.
So why, then, do medical charges and prices bear little resemblance to fair market value? In other words, when we receive a medical bill or statement in the mail, we typically see that, although our provider charged $1,000 for a service, she seemed content with receiving $250 as payment in full.
Why does the medical care industry work this way? The reasons for this are twofold. First, as the U.S. health care system grew rapidly following World War II, the industry was largely organized as non-profit. As the industry expanded, policymakers put more pressure on non-profit entities to show that they were providing sufficient levels of “charity” care (or alternatively carrying sufficient levels of “bad debt”) to justify their tax-exempt status; that is, charity care and bad debt were consider forms of “community benefit.” One way for hospitals and other health care entities to report high levels of charity care was to keep their charges high, negotiate lower rates on a per case basis, and classify the difference as either charity care of bad debt. Although the industry now contains a mix of non-profit and for-profit entities, such pricing behavior has largely continued. Second, health care entities generally find it more effective to bargain and adjust from an arbitrarily high “chargemaster” (i.e., “price list”) rather than a price list more reflective of fair market value.
This raises two questions. First, what is the meaning and interpretation of reasonable and fair market value? And second, how do sellers (or providers) determine what to accept as payment in full? Beginning with the first question, a helpful way to consider a reasonable value is to think of the concepts of supply and demand, which are core tenets of economic theory. Supply and demand are based on two inputs: price and quantity. The demand “curve” maps various combinations of prices and quantities that we might observe in a market. It represents the amount that consumers are “willing to pay” for a given quantity of a good or service. Similarly, the supply curve maps the various combinations of prices and quantities observed in the market and reflects the price at which suppliers are “willing to supply” for a given quantity of a good or service.
The intersection of the supply and demand curves represents the market “equilibrium.” In practice, this is not an exact point, but rather a range of prices and range of quantities. Prices in this equilibrium range represent the prices at which products and services are commonly transacted in the marketplace, and in economics-related fields this is considered equivalent to fair market value and reasonable value. As an example, consider the market for brewed coffee. Retail prices typically range from $2-$5 per cup. The implication of this is that consumers are willing to pay $2-$5 per cup, and suppliers are willing to supply brewed coffee at $2-$5 per cup; consequently, the fair market value and reasonable value of a cup of brewed coffee is $2-$5, which is also equal to the range over which brewed coffee is transacted. If a café were to offer a regular cup of brewed coffee for $100, it is unlikely that it would sell. Thus, we could not reasonably argue that the cup of coffee is valued at $100, or “worth” $100, if no consumers purchase it at that price. Of course, many industries are more complicated and nuanced than the market for brewed coffee, but this same basic illustration is relevant for all industries.
The second way in which fair market value and reasonable value can be interpreted is focused on the supply side of the supply-demand relationship. As I discussed above, there is typically a range of prices over which a supplier is willing to supply the market. In the medical care market, this can be thought of as equivalent to the amount that providers are willing to accept as payment in full. It would also be equivalent to the price at which the product or service is typically transacted. If we were plot these prices on a horizontal axis, and record the frequency of transactions at each price, the result would be a “normal” curve or “bell-shaped” curve like the one shown in Figure 1. Any point along this curve can be thought to represent an actual observed price (or charged or billed amount).
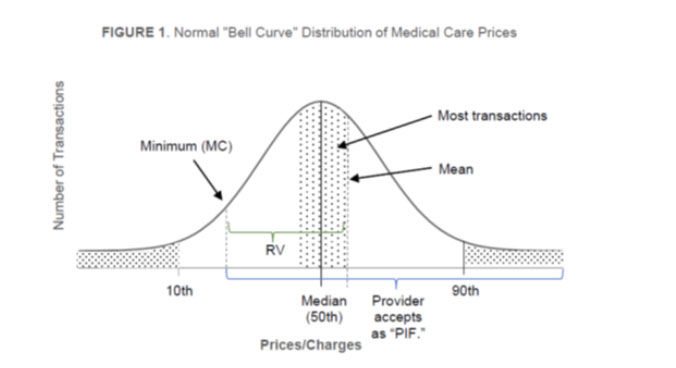
Figure 1 shows the median (50th percentile) in the center of the distribution, with an equal number of transactions above and below the median. The figure also shows the 90th percentile on the right (i.e., higher prices) and the 10th percentile on the left (i.e., lower prices). In medical care, statistical means (i.e., averages) are typically somewhat higher than medians because “outliers” are typically on the higher end of the distribution (i.e., most providers do not typically charge excessively low charges). The shaded area around the median depicts the range of “equilibrium” prices as described above in the context of the intersection of supply and demand; more importantly, this represents the region wherein most transactions take place. It is also likely that most providers will have a “minimum” charge that they will accept as payment in full. The minimum price typically represents the point at which the provider’s marginal costs (“MC”) are “covered;” that is, the point at which they are still able to earn positive margins given the practice’s cost structure. This hypothetical minimum is shown to the left of the equilibrium price range.
The implication of this is that a rational provider will accept as “payment in full” (“PIF”) amounts equal to the range of prices indicated by the “PIF” bracket. Of particular importance here is that providers will accept as PIF amounts less than the median, so long as those amounts are higher than the minimum, where MC is covered. In businesses with high fixed costs (like hospitals and medical care practices), it makes sense to accept amounts as low as MC, because such amounts are still associated with positive operating margins. However, in businesses with high fixed costs (such as health care facilities), MC will typically be less than average costs (“AC”), and AC will be less than the median charges. Thus, the PIF acceptance range will include the median and below, as indicated. In practice, think about how the space and equipment a provider must have in place to simply treat one patient. It is in their interest to treat as many people as possible accepting as PIF amounts as low as their MC. Again, this implies that a rational provider will accept as PIF amounts equal to or less than the median. Reasonable value is indicated by the upper (green) bracket. Based on the discussion above, it follows that reasonable value is defined as: MC ≤ RV ≤ Median Charge.
As a final note, even in the absence of coverage, it is widely known that individuals can negotiate with health care providers. Most providers will accept as PIF amounts equal to or even lower than fair market or reasonable value (as discussed above) and are likely to accept, as payment in full, amounts as low as their marginal costs (i.e., the lowest amount at which they can “cover” their costs). In other words, as discussed above, RV ≥ MC, which means that providers will not “lose money” by accepting the RV amount; indeed, they could accept much less than the median and still earn a profit.
(John Schneider, PhD, and Cara Scheibling, MBA)


